


Endometriosis
Endometriosis is a chronic inflammatory condition affecting 6 to 10% of women. It is a condition whose main symptoms are characterised by quite debilitating pain, particularly during menstruation, and which can also lead, in a certain percentage of cases, to infertility issues.
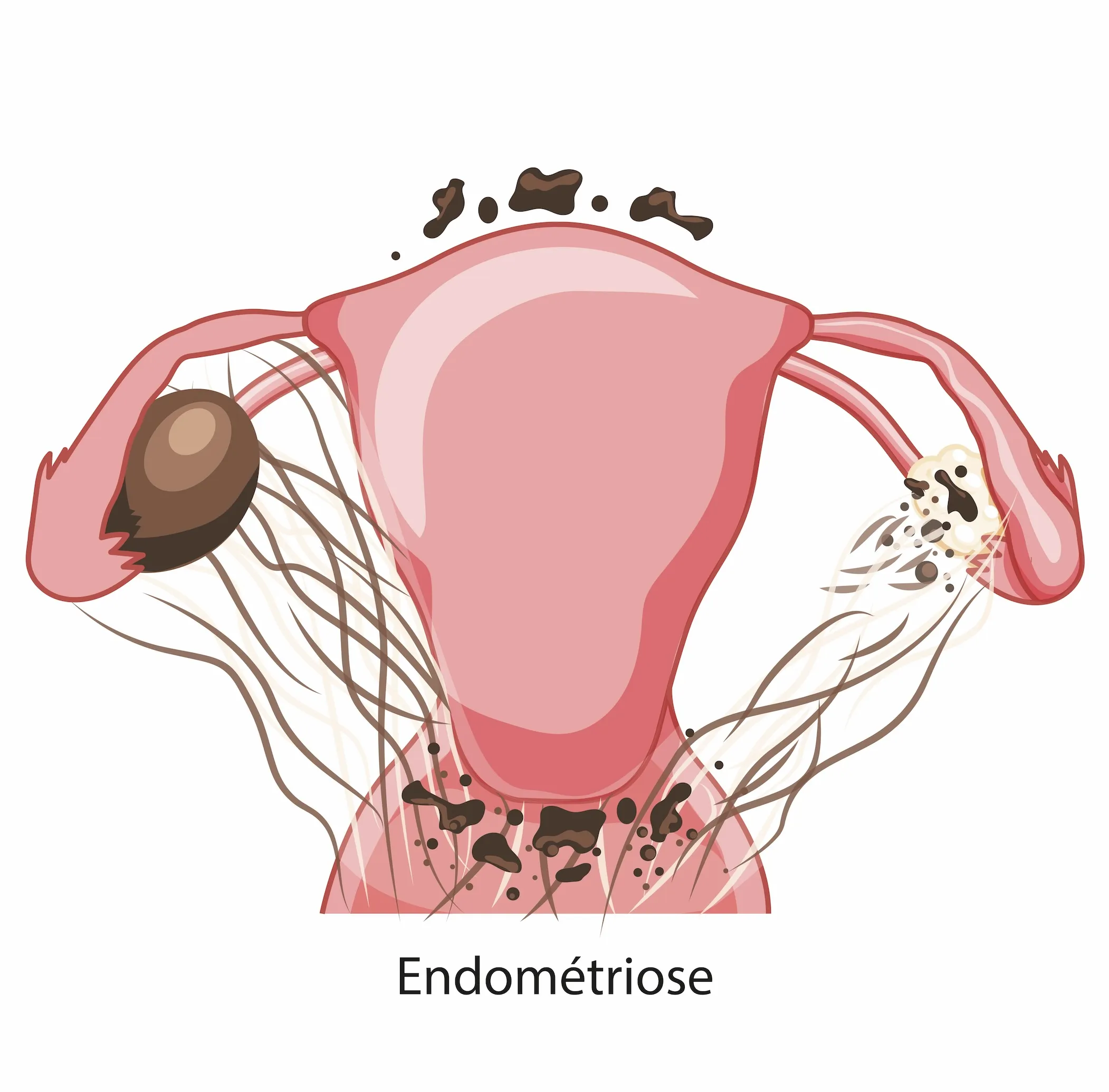
Endometriosis primarily affects the pelvic region, but can spread beyond the gynaecological organs—namely the ovaries, fallopian tubes and uterus.
It also affects neighbouring organs, namely the digestive system and, in some cases, the urinary system.
The condition tends to affect a variety of organs. It is for this reason that the multidisciplinary approach and the expertise of digestive surgeons, urologists, gastroenterologists and radiologists in diagnostic procedures were the driving force behind the launch of this project.
As for treatment options, the team is further strengthened by the presence of a pain management anaesthetist, a nutritionist and a psychologist
Two separate teams meet monthly:
- The first comprises gynaecologists, surgeons and radiologists to discuss medical and surgical management.
- A second team comprising the pain specialist, physiotherapist, psychologist, nutritionist, internist and gynaecologists to extend the assessment of chronic pelvic pain beyond endometriosis and provide comprehensive management.
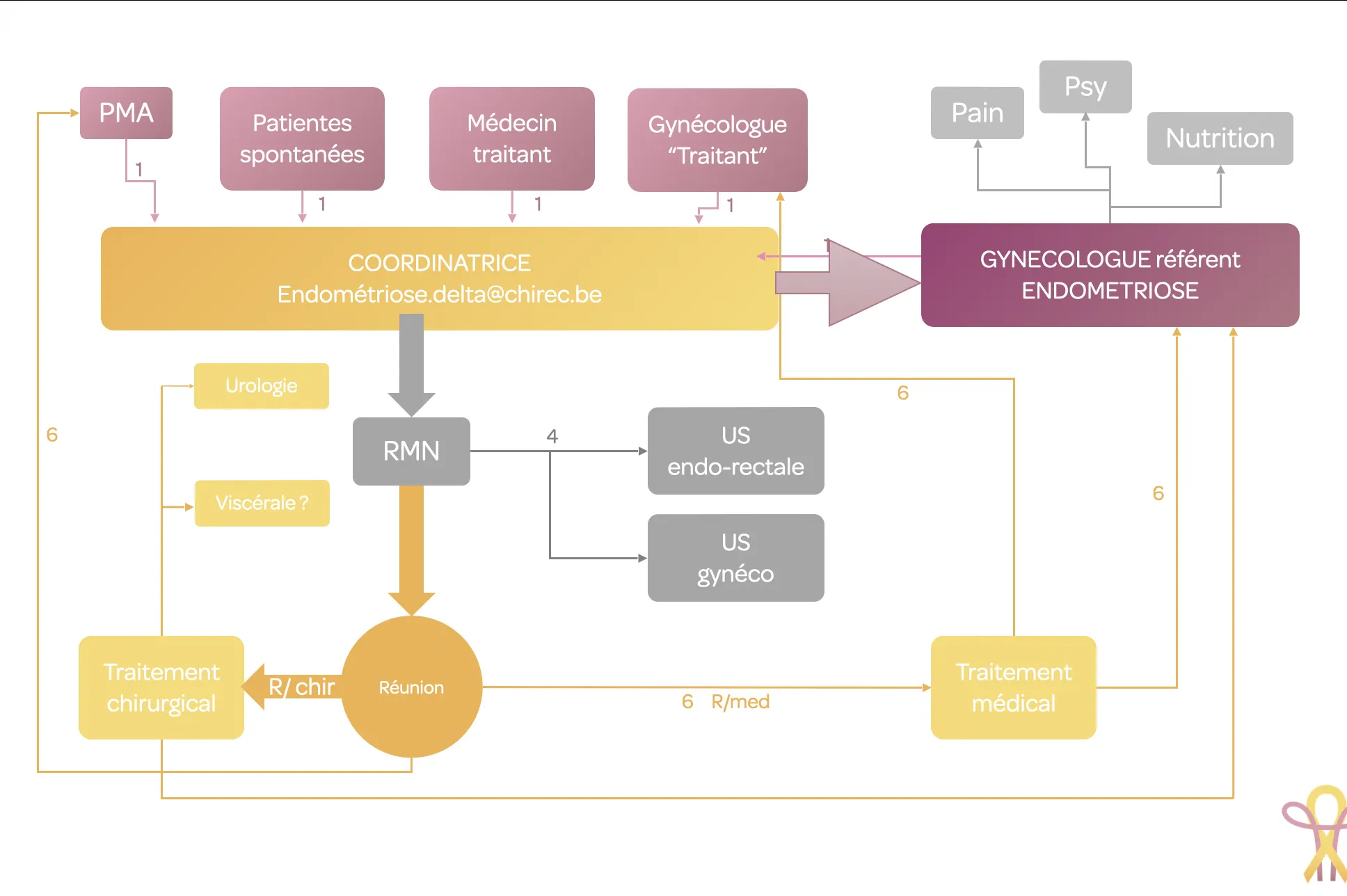
We have designed a care pathway that offers patients rapid treatment. This pathway includes additional tests that will facilitate consultation and enable treatment proposals to be formulated within a relatively short timeframe.
Our work: One-year review
A first in Belgium
Cryoablation of endometriosis nodules in the abdominal wall
The team
Within a dedicated multidisciplinary team, the gynaecologist plays a central role in the management of endometriosis.
In collaboration with specialists such as radiologists, surgeons, pain specialists and psychologists, the gynaecologist coordinates the key stages of diagnosis and treatment.
Thanks to their expertise, they ensure personalised follow-up for each patient, from the first symptoms to the implementation of a tailored care plan.
This integrated approach enables the provision of comprehensive solutions, including medical, surgical and supportive treatments, to significantly improve patients’ quality of life and meet their specific needs.
Transvaginal ultrasound is an essential diagnostic tool for assessing endometriosis.
This technique allows for the precise visualisation of the internal structures of the pelvic region and the identification of lesions characteristic of endometriosis, such as ovarian cysts and deep nodules.
Transvaginal ultrasound thus enables early detection and a detailed assessment of the location and extent of lesions, key factors in tailoring treatment to each patient. This type of ultrasound is therefore an essential step towards a reliable diagnosis and personalised management of endometriosis.

Our gynaecologists
Medical Coordinator of the clinic - Gynaecologist

Gynaecologist

Gynaecologist

Gynaecologist

Gynaecologist

OUR ULTRASOUND SPECIALIST
Transvaginal ultrasounds

Endometriosis and infertility are two closely linked conditions. It is estimated that endometriosis is present in over 50% of infertile women.
The mechanisms of endometriosis involved in infertility are numerous and controversial.
These range from disorders of ovulation and fertilisation, through defects in gamete transport, to problems with embryo implantation.
It is, in fact, adenomyosis—a specific form of endometriosis affecting the uterine muscle—that can disrupt embryo implantation in the uterine cavity.
Other purely mechanical phenomena linked to endometriosis may be involved in infertility, such as peritubal-ovarian adhesions or adnexal lesions hindering the progression of spermatozoa through the female tract to allow for optimal fertilisation.
Many questions remain unanswered regarding the management of endometriosis in cases of infertility.
Management by a multidisciplinary team (gynaecological surgeons, radiologists, assisted reproductive technology specialists, gastrointestinal surgeons, etc.) therefore remains a key factor in resolving fertility issues in patients with endometriosis.
However, the decision on treatment, whether surgical or medical, must always be made in consultation with the couple.
Indeed, the role of surgery and in vitro fertilisation treatments is constantly reassessed on a case-by-case basis to ensure patients receive the best possible care.
The role of the endometriosis clinic will enable comprehensive care, from endometriosis symptoms to fertility issues.
In fact, for several years now, there has been a reimbursement scheme from private health insurers that allows for the preservation of oocytes for patients with certain types of endometriosis.
OUR FERTILITY SPECIALIST (Assisted Reproductive Technology)
Gynaecologist, fertility specialist (Assisted Reproductive Technology)

MRI (magnetic resonance imaging) plays a fundamental role in the management of endometriosis.
It is the most effective technique for detecting endometriosis lesions, particularly deep endometriosis (uterine torus, uterosacral ligaments, vagina and rectum), which correlates with the severity of pain and infertility.
This tool enables the specialist radiologist to produce a precise map of the lesions, which is essential for planning surgical treatment.
It is a non-invasive examination; the patient lies in the scanner for 15–20 minutes, following prior preparation (a 4-hour fast and a rectal enema) to avoid any artefacts that might interfere with image interpretation.
The rectal enema involves injecting a solution into the rectum (Cleen Enema®) using a small bulb syringe (see instructions on the leaflet), to be carried out by the patient 1–2 hours before the examination or the evening before.
This product will induce the urge to have a bowel movement after a few minutes in order to empty the rectum, which is the distal part of the digestive tract.
This step helps to obtain much higher quality MRI images and allows for optimal analysis of the scan.
Our radiologists
Radiologist - Head of Department

Radiologist

Radiologist

Involvement of the digestive tract is the most common non-gynaecological site of endometriosis.
The most commonly affected areas include the rectum, the sigmoid colon, as well as the distal small intestine, the caecum and the appendix, although the latter are less frequently affected (< 10%). In contrast, organs such as the stomach, the duodenum, the liver and the spleen are never affected.
Endometriosis lesions may be single (70%) or multiple (30%) and vary in depth. They may be superficial, affecting only the serosa, or deep, infiltrating the muscular and submucosal layers of the digestive tract wall. Most deep nodules do not reach the mucosa, making them difficult to detect during a colonoscopy.
Symptoms vary considerably from one patient to another and may include diarrhoea, abdominal cramps, pain during bowel movements, constipation, and bloating, often exacerbated during menstruation. Anal bleeding (rectal haemorrhage) is rarely caused by endometriosis nodules.
Treatment generally begins with medical management, with amenorrhoea often proving beneficial. If necessary, surgery is considered, using techniques such as shaving for superficial nodules or more extensive approaches for deeper lesions. The choice of surgical method depends on imaging assessment, including pelvic MRI and rectal echoendoscopy.
Risks associated with surgery include haemorrhage, damage to surrounding organs, and various post-operative complications such as fistulas or abscesses, sometimes requiring further procedures.
Our gastrointestinal surgeons
Deputy Medical Coordinator – Gastrointestinal Surgeon

Gastrointestinal Surgeon

Rectal echoendoscopy (REE) enables an endoscopic examination and an ultrasound assessment of the anatomical structures located in the immediate vicinity of the probe.
In the management of deep pelvic endometriosis, REES is a second-line investigation.
It enables a definitive diagnosis of ‘gastrointestinal parietal endometriosis’ to be made when rectal and/or sigmoid infiltration has been identified, most commonly via MRI.
In this context, ER with a rigid probe is preferable, as pelvic gastrointestinal involvement is most commonly located in the upper rectum, extends to the rectosigmoid junction in approximately 30% of cases, and is accompanied by a second sigmoid site in nearly 15% of cases.
For patients for whom resection is proposed, ERCP makes an indispensable contribution to the pre-operative staging assessment.
ERCP can determine the presence and extent of gastrointestinal involvement, which is usually located in contact with the insertion of the uterosacral ligaments, the torus, or the left ovary.
ER helps determine the choice of surgical technique and the procedure to be performed on the digestive tract.
It is carried out following a cleansing enema to be administered the day before and on the day of the examination. Preferably under propofol and in the left lateral decubitus position. The examination is estimated to take 30 minutes.
Our gastroenterologists
Gastroenterologist

Gastroenterologist

Gastroenterologist

Involvement of the urinary tract accounts for less than 1% of endometriosis lesions.
These lesions can vary in location, size and impact on health.
The urologist is involved in the diagnosis, prescribing any necessary additional tests (ultrasound, MRI, cystoscopy, urodynamic assessment), and in surgical treatment if required.
They also use simple pre-operative procedures to facilitate complex interventions (JJ stent).
Our urologist
Urologist

The internist carries out a thorough analysis of your entire system, seeking to identify the subtle links between the body’s various organs and systems. A central aspect of this assessment is the study of the gut-brain axis, which links digestive function to neurological and hormonal responses. This provides a better understanding of the impact of endometriosis on your overall well-being.
The internist’s approach is not limited to treating the symptoms of endometriosis, but aims to restore the body’s overall balance. Through a comprehensive assessment, they develop a personalised care plan that incorporates recommendations on diet, physical activity and stress management, as well as appropriate medical treatments.
This holistic approach allows for a more comprehensive treatment of endometriosis, taking into account all the factors influencing your health.
Our General Practitioner
General Practitioner

Pain associated with endometriosis takes various forms:
- Secondary visceral pain.
- Neuropathic pain.
- Secondary musculoskeletal pain.
- Subacute or chronic post-operative pain.
The pain specialist:
- Assesses the pain: intensity, location, type of pain (timeline, history).
- Assesses the functional and psychosocial impacts of the pain.
- Proposes a management plan addressing the various aspects of the pain: medication, non-pharmacological interventions (physiotherapy, psychology, nutrition, etc.) and, where appropriate, injections.
- Pre-operatively, the pain specialist develops a strategy to identify the risk of pain becoming chronic, and proposes preventive management before the procedure where possible, followed by post-operative management.
- Communicates and collaborates with the various healthcare professionals (gynaecologists, psychologists, physiotherapists, etc.).

Our anaesthetist - pain specialist
Pain specialist

As part of a comprehensive approach to managing endometriosis, sexology helps address its intimate, emotional and relational consequences. This discipline aims to understand sexuality, identify potential difficulties (pain, reduced desire, anxiety, altered body image) and seek appropriate solutions.
During a consultation, a sexologist will explain the mechanisms of pain and its effects on the individual and intimacy, and suggest positions or practices to reduce discomfort, recommend relaxation or breathing exercises, and offer advice on improving communication within the couple.
The aim is to help restore confidence, reduce anxiety related to sexual intercourse, and rediscover a more fulfilling sex life despite the presence of endometriosis.
As part of the medical treatment for endometriosis, sex therapy thus helps to improve quality of life, emotional well-being and relationship satisfaction.
Sexologist

Sexologist

Physiotherapy offers valuable support for people with endometriosis.
Through gentle, targeted work, physiotherapy helps to release adhesions and restore flexibility to the pelvic structures, promoting greater comfort in daily life.
In addition, it also supports the management of anxiety and stress, often exacerbated by chronic pain, by promoting relaxation and a renewed sense of bodily awareness.
Whether to reduce symptoms, improve quality of life or facilitate a return to daily activities, physiotherapy is an essential pillar of the multidisciplinary management of endometriosis.
Our physiotherapist
Physiotherapist
Specialising in endometriosis, the dietitian helps you adapt your diet to better manage inflammation, alleviate pain and improve your gut comfort.
She takes into account your eating habits and lifestyle to suggest targeted, realistic adjustments tailored to your daily life.
Taking a holistic approach, the dietitian also offers advice on how to better manage stress, improve sleep quality and boost your vitality.
Every support programme is personalised: the aim is to work with you to build lasting changes that respect your tastes and your lifestyle.
This nutritional support provides genuine complementary assistance to other treatments, helping to improve your quality of life and daily well-being.
Our dietitian
Dietitian

Our psychologist
Psychologist
Contact us
Coordinating Secretary – Book appointments by phone :

Secretary – Book appointments by phone :